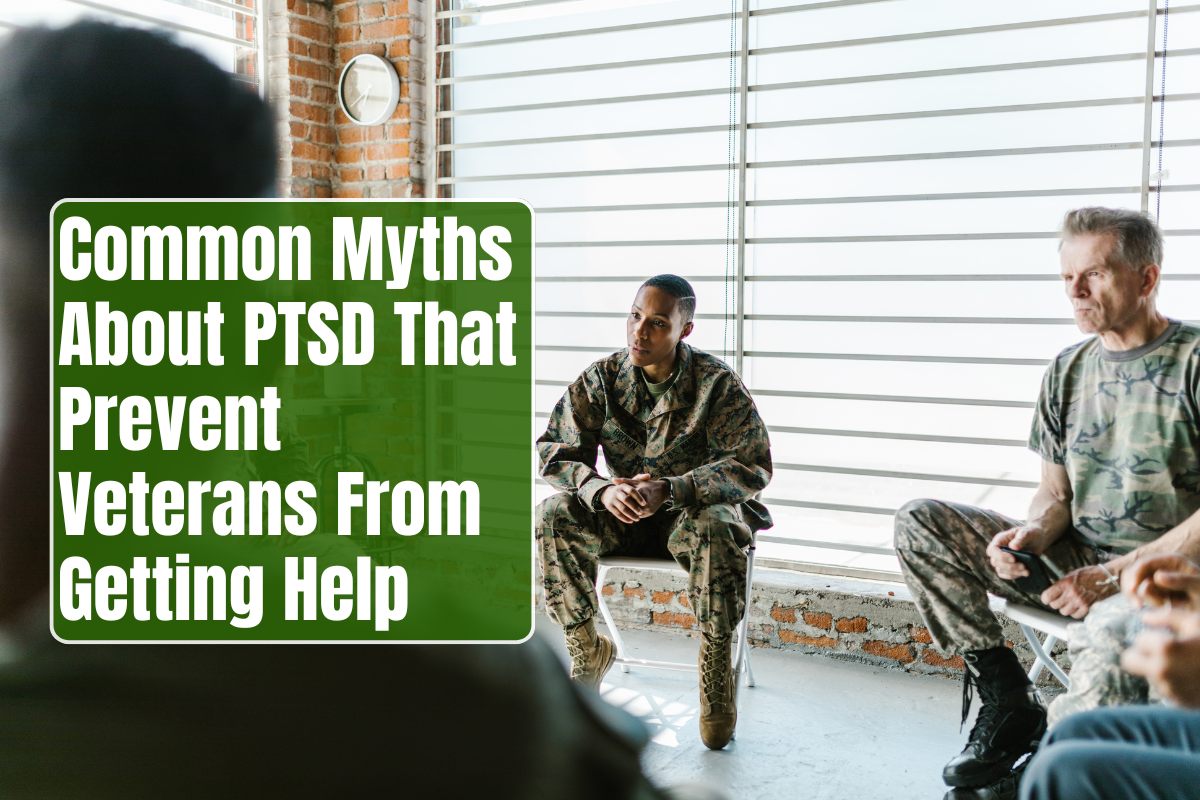
Post-traumatic stress disorder (PTSD) is one of the most prevalent yet misunderstood mental health conditions affecting military veterans. Despite decades of awareness, misconceptions still prevent thousands from seeking the help they need. These myths not only perpetuate stigma but also reinforce silence, worsening symptoms and straining families. Dispelling misinformation is vital to ensuring that veterans feel safe, respected, and empowered to begin their healing journey.
Understanding PTSD Beyond the Stereotypes
PTSD develops after exposure to life-threatening or traumatic events such as combat, assault, or severe accidents. Among U.S. and allied military veterans, studies indicate that up to 30% from combat zones experience PTSD at some point. Symptoms range from flashbacks and nightmares to avoidance, guilt, anxiety, and emotional numbness.
While PTSD is a medical and psychological condition, not a moral failing, numerous myths continue to distort public and personal understanding—creating barriers to care. Recognizing the truth behind these myths helps challenge false beliefs and encourage recovery.
Myth 1: “PTSD Means You’re Weak or Can’t Handle Stress”
Reality: This is perhaps the most damaging myth. PTSD has nothing to do with strength, bravery, or willpower. It is a natural reaction of the brain and body to overwhelming trauma.
Military training conditions soldiers to be resilient and composed under pressure, but no amount of discipline can erase biological stress responses. Combat, loss, and violence alter the brain’s fight-or-flight system, leaving it stuck in overdrive. PTSD reflects injury, not inadequacy.
Acknowledging distress is a sign of self-awareness, not weakness. Seeking treatment is an act of courage—choosing to fight for wellness rather than suffer in silence.
Myth 2: “Only Combat Veterans Get PTSD”
Reality: PTSD affects veterans and civilians alike, regardless of battlefield service. In the military, PTSD can stem from a wide variety of experiences—sexual violence, training accidents, moral injury (guilt over combat decisions), or witnessing others’ suffering.
Many service members develop symptoms after non-combat trauma, including military sexual assault (MST), which affects both men and women. According to the VA, one in three women and one in fifty men report MST, though numbers may be higher due to underreporting.
Limiting PTSD to combat experiences invalidates countless veterans who struggle without recognition or resources.
Myth 3: “You’ll Never Get Better—PTSD Lasts Forever”
Reality: While PTSD can be chronic, it is highly treatable. Evidence-based therapies—such as Cognitive Processing Therapy (CPT), Prolonged Exposure (PE), and Eye Movement Desensitization and Reprocessing (EMDR)—yield significant symptom reduction in 60–90% of patients.
Many veterans achieve full recovery or long-term remission. Healing takes time and support, but the outcomes are overwhelmingly positive when individuals seek early intervention.
Untreated PTSD can persist, but with therapy, medication, peer support, and healthy lifestyle adjustments, veterans regain function, relationships, and optimism.
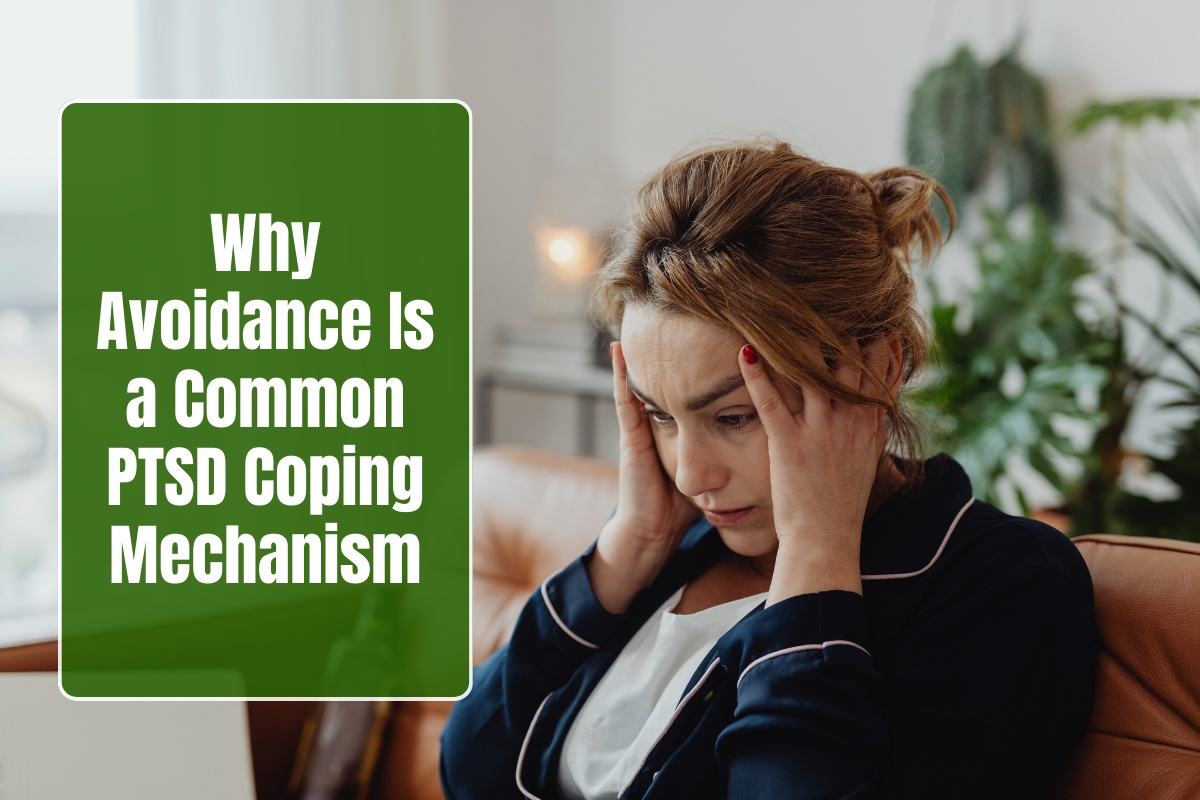
Myth 4: “If You Talk About It, You’ll Relive It and Make It Worse”
Reality: Avoidance is a hallmark symptom of PTSD, and many veterans fear therapy will reopen wounds. However, treatment methods are designed to guide exposure safely and gradually—helping the brain process and organize traumatic memories rather than relive them.
In therapies like PE or EMDR, licensed clinicians create controlled environments for veterans to confront and reframe memories, reducing their emotional charge. Over time, triggers lose power and confidence grows. Silence, not conversation, deepens suffering; talking about trauma is how recovery begins.
Myth 5: “Getting Help Will Hurt My Career or Reputation”
Reality: Fear of professional consequences remains a major barrier to treatment, especially among active-duty and veteran communities. However, confidentiality laws protect mental health information. Seeking therapy does not automatically affect security clearances or employment.
The Department of Defense and VA actively encourage early mental health care, emphasizing that untreated PTSD poses greater risks—to a person’s performance, relationships, and overall well-being—than seeking assistance ever could.
Stigma is fading as more veterans, leaders, and public figures openly share their stories, proving that compassion and courage are redefining what “strength” truly means.
Myth 6: “PTSD Makes People Violent or Dangerous”
Reality: Hollywood often portrays veterans with PTSD as aggressive or unstable, but this stereotype couldn’t be further from reality. PTSD does not inherently make a person violent.
While some individuals may display irritability or anger—common stress reactions—most manage emotions safely or seek constructive outlets. In fact, veterans with PTSD are more likely to harm themselves through despair or withdrawal than others.
Labeling sufferers as dangerous fuels discrimination, isolating them from the support they need. Compassionate understanding—not fear—is the correct response.
Myth 7: “Therapy and Medication Don’t Work”
Reality: Modern PTSD treatment blends evidence-based psychological therapy with optional medication support. Cognitive-behavioral therapies restructure negative thought patterns; EMDR helps desensitize trauma responses; medications like SSRIs stabilize mood and sleep.
VA studies show that consistent treatment drastically reduces symptoms and enhances quality of life. Moreover, new options—such as telehealth, virtual reality exposure therapy, and family-inclusive programs—bring care closer and more effectively than ever. Recovery success depends more on persistence and connection than on any single method.
Myth 8: “Veterans With PTSD Should Handle It Alone”
Reality: Military values of self-reliance often discourage veterans from seeking help, but healing from trauma requires connection, not solitude. Social support—family, peers, and therapy groups—acts as one of the strongest protective factors against relapse and suicide.
Veterans who join group therapy or engage with peers often express comfort in realizing they’re not alone. Shared experience reduces shame and fosters mutual accountability, making recovery sustainable in the long term.
The Power of Awareness and Education
Dispelling PTSD myths transforms families and communities. When misconceptions fade, empathy rises. Families learn to respond with patience instead of fear; workplaces adopt supportive policies; society honors service not with pity, but with partnership.
Education campaigns, veteran storytelling projects, and open dialogues within organizations are powerful antidotes to stigma. Each conversation chips away at the silence that keeps trauma in control.
FAQs
Q1: Is PTSD a sign of weakness?
No. PTSD is a medical response to trauma, not a personal failure. It reflects how the brain processes overwhelming experiences.
Q2: Can veterans fully recover from PTSD?
Yes. With early and consistent treatment, most achieve major symptom reduction or remission, regaining emotional stability and quality of life.
Q3: Does therapy make PTSD worse before it gets better?
Therapy may temporarily evoke emotions, but it’s designed to relieve—not intensify—trauma. Controlled exposure enables long-term healing.
Q4: Is PTSD only caused by combat?
No. Causes include assault, accidents, or witnessing trauma. Many military sexual trauma survivors develop PTSD outside combat settings.
Q5: Does seeking mental health care affect military or VA benefits?
In most cases, no. Confidentiality laws protect veterans, and seeking help demonstrates responsibility and readiness to recover.
Q6: How can families challenge these myths?
By learning about PTSD through VA or veteran support resources, speaking openly, and reassuring loved ones that asking for help reflects true strength.