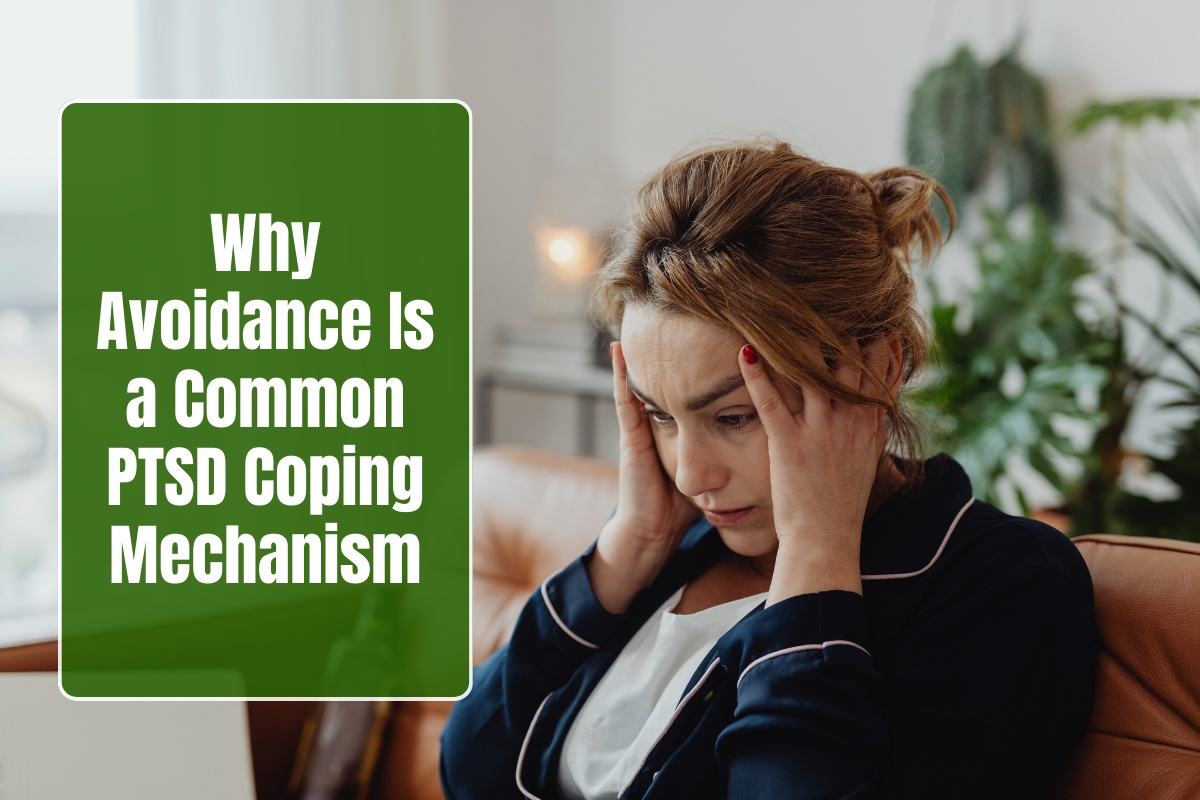
Living with a partner experiencing PTSD imposes a profound emotional toll on spouses, manifesting as secondary trauma, chronic stress, and eroded well-being that often goes unrecognized. Partners absorb the fallout of symptoms like emotional numbing and hyperarousal, leading to their own anxiety, depression, and isolation, yet targeted support can mitigate these effects. Understanding this burden fosters empathy and prompts families to seek joint resources for resilience.
Secondary Traumatization and Symptom Absorption
Partners develop PTSD-like symptoms from prolonged exposure to their veteran’s trauma reactions, a phenomenon known as secondary traumatization affecting up to 50% of spouses in some studies.
They experience intrusive thoughts, hypervigilance, and nightmares mirroring the veteran’s, compounded by direct exposure to outbursts or withdrawal. This indirect trauma erodes emotional reserves, leaving partners in a perpetual state of alertness, scanning for triggers to prevent escalation.
Research on wives of war veterans shows half exhibit six or more secondary stress symptoms, including emotional exhaustion and sleep disturbances, far exceeding general population rates. Male partners of female veterans report parallel isolation and lowered life satisfaction, underscoring the bidirectional impact regardless of gender.
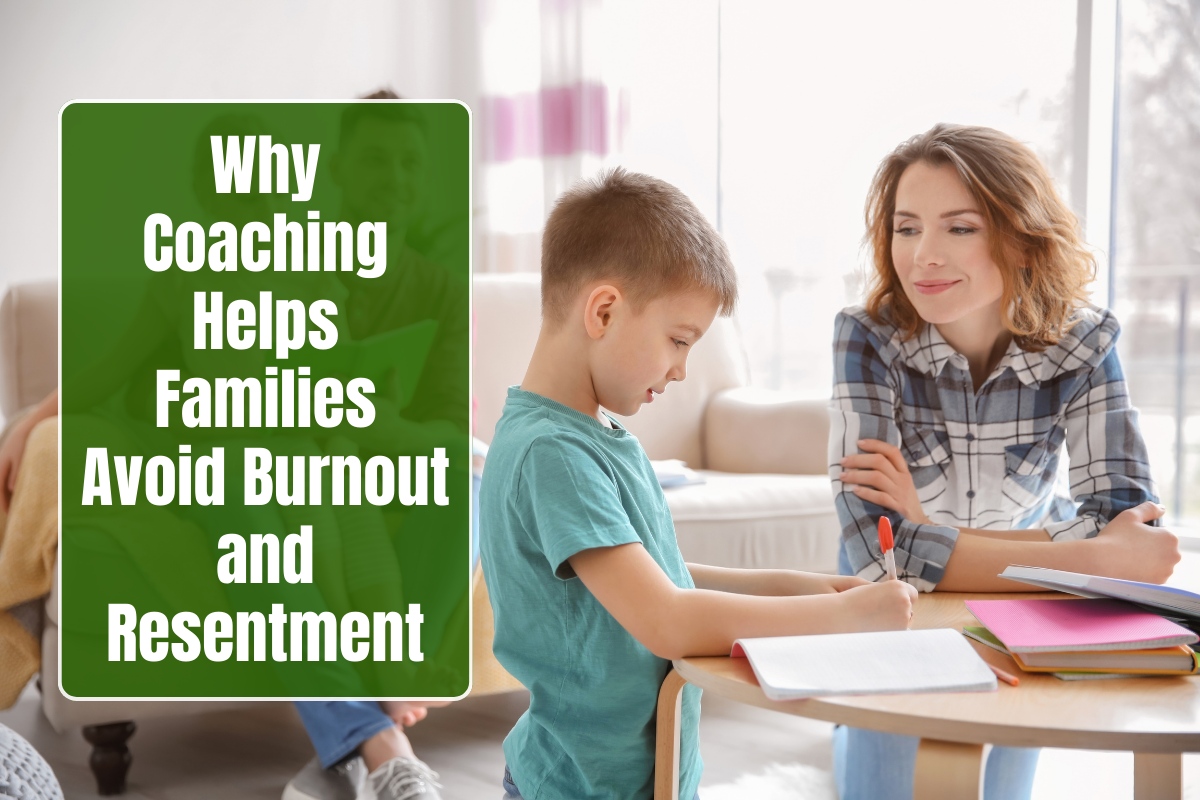
Caregiver Burden and Role Overload
Spouses shoulder disproportionate household, childcare, and financial responsibilities, averaging 9.6 hours daily for 6.4 years, resulting in Zarit Burden scores well above clinical thresholds (average 21.8).
This overload breeds resentment as personal needs—hobbies, friendships, self-care—fade, with 84% reporting high stress and 33% meeting depression criteria. Partners constantly monitor and accommodate PTSD triggers, like avoiding crowds or topics, which amplifies feelings of entrapment.
Financial strain compounds emotional fatigue, with 60% struggling to pay bills and 44% lacking insurance, intensifying helplessness amid the veteran’s potential unemployment. Qualitative accounts reveal “chronic sorrow” and “defeat,” as partners grieve the pre-PTSD relationship while managing daily chaos.
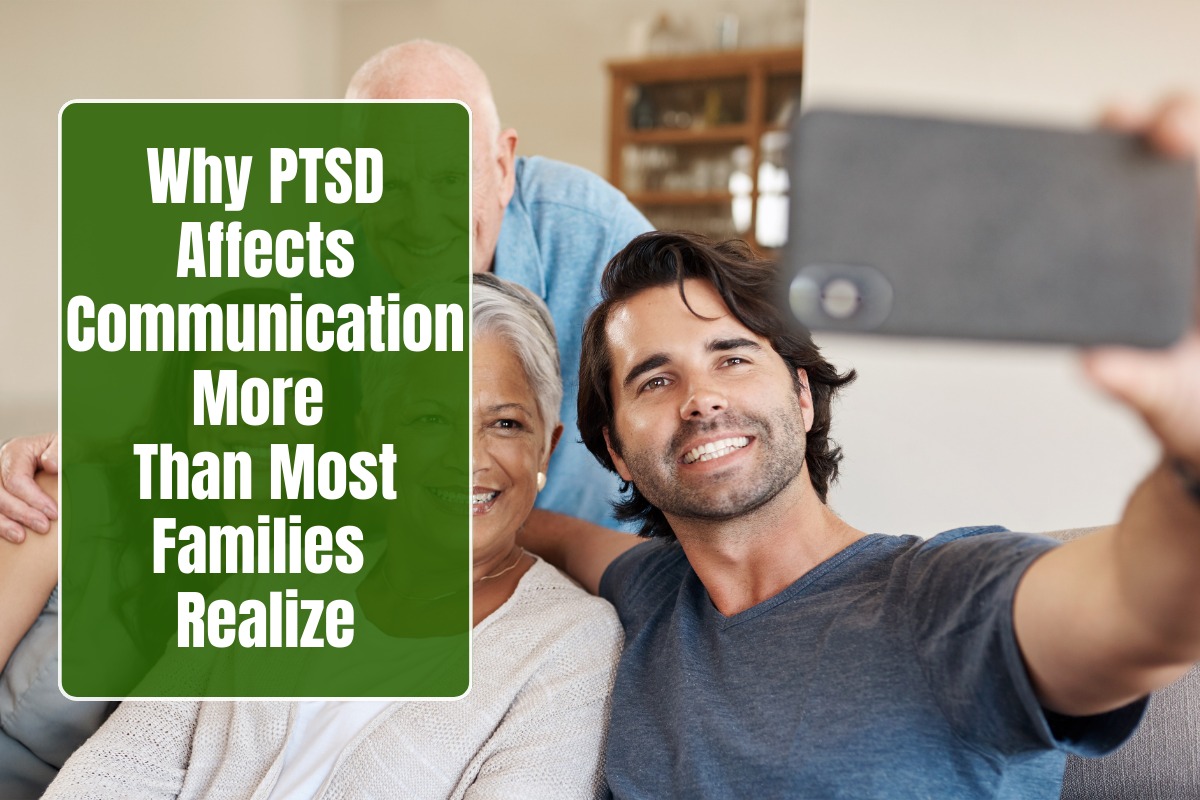
Erosion of Intimacy and Relationship Satisfaction
Emotional numbing in veterans uniquely predicts partners’ dissatisfaction with intimacy and shared activities, creating profound loneliness despite cohabitation. Partners desire more affection and engagement, yet face rejection-like detachment, leading to sexual dysfunction worries and emotional starvation. Conflict escalates during discussions, with both displaying heightened hostility and reduced humor or acceptance, perpetuating cycles of blame.
Vietnam-era data confirms partners report lower relationship quality, more marital troubles, and intimacy fears compared to non-PTSD counterparts. This fosters ambiguous loss—mourning the “lost” partner—while navigating volatile dynamics, often resulting in social withdrawal.
Psychological Distress: Anxiety, Depression, and Isolation
Depression and anxiety surge, with partners scoring high on CES-D scales (average 11.5) and manifesting mood disorders at rates double those of civilian spouses. Living in a “volatile environment” triggers constant eggshell-walking, fostering defeat, anger, and spiritual pain from unmet emotional needs. Loneliness intensifies as partners lose peer networks, feeling alienated by the all-consuming PTSD focus.
High-burden cases highlight role strain, where even veteran spouses reverse caregiving roles yet face communication breakdowns and identity loss. Somatic complaints like pain syndromes emerge alongside dissociative tendencies from chronic absorption of trauma.
Long-Term Health and Identity Shifts
Prolonged toll manifests physically—headaches, insomnia—and psychologically, with shifts in self-perception from empowered to burdened caregiver. Partners report inequality in relationships, losing congruence with their pre-caregiving identity, which hampers personal growth. Without intervention, this leads to burnout, with studies urging family-inclusive treatments to prevent intergenerational trauma.
Support Pathways for Partners
VA caregiver programs offer respite, counseling, and financial aid, while therapies like CBCT address dyadic distress. Peer groups validate experiences, reducing isolation; self-care routines and boundaries preserve partners’ health. Early recognition via screenings empowers spouses to reclaim agency amid the toll.
FAQs
Q1: What is secondary traumatization in partners?
Indirect PTSD-like symptoms from absorbing veteran’s trauma reactions, affecting up to 50% with intrusions, hypervigilance, and exhaustion.
Q2: How does caregiver burden manifest daily?
Overload from 9+ hours of tasks, trigger management, and unmet needs, yielding high stress (84%) and depression (33%).
Q3: Why does intimacy suffer most?
Veteran’s emotional numbing blocks closeness, prompting partners’ desires for change and feelings of rejection.
Q4: Do partners develop their own mental health issues?
Yes, elevated anxiety, depression, and mood disorders double civilian rates, plus somatic pain and isolation.
Q5: How common is financial and social strain?
60% face bill troubles, 44% lack insurance; social withdrawal heightens loneliness.
Q6: What support helps partners cope?
VA respite/counseling, peer groups, CBCT therapy, and self-care boundaries reduce burden effectively.