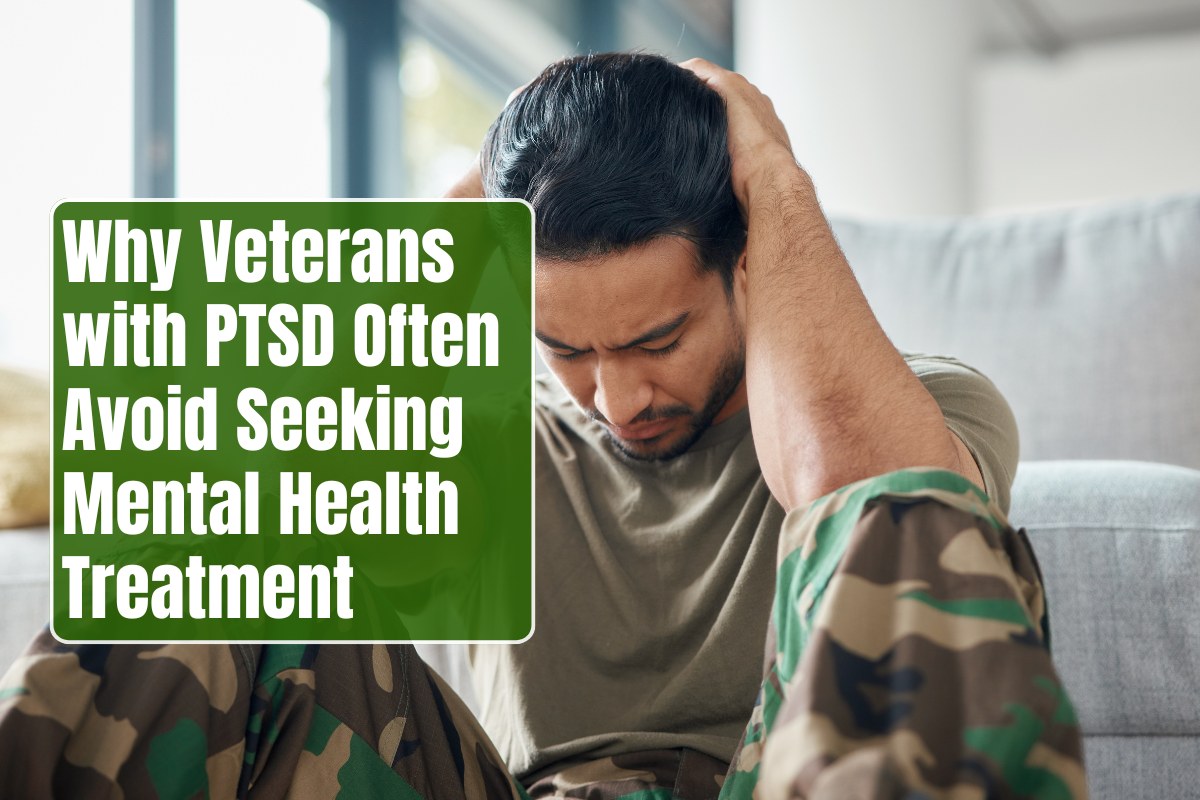
Veterans with PTSD frequently delay or avoid mental health treatment despite severe symptoms, with studies showing only 22-40% of those affected seeking care due to intertwined personal, cultural, and systemic obstacles. These barriers perpetuate suffering, elevate suicide risks, and strain families, yet understanding them can guide targeted interventions like stigma-reduction campaigns. Overcoming avoidance requires reframing help as strength aligned with military resilience.
Stigma and the “Weakness” Perception
Military culture emphasizes toughness and self-reliance, leading veterans to view mental health treatment as an admission of weakness or failure. Perceived public stigma—fearing judgment from peers, family, or commanders—ranks among top barriers, with 60% of personnel citing concerns about being labeled “crazy” or unreliable. Self-stigma internalizes these views, fostering shame that discourages disclosure even to close ones.
Veterans often endorse stereotypes more harshly against themselves than peers, believing treatment signals character defects despite knowing it aids recovery. This disconnect delays care, as seen in surveys where stigma triples non-attendance rates for trauma-focused therapies. Active-duty fears of career derailment amplify avoidance, with personnel hiding symptoms to protect promotions or deployments.
Distrust in Treatment Effectiveness
Many veterans doubt therapy works, believing PTSD symptoms represent permanent damage rather than treatable conditions. Negative beliefs like “talking won’t help” or “medication changes who I am” stem from misinformation or past ineffective encounters, leading to premature dropout. Only half express confidence in improvement, correlating directly with utilization gaps.
Knowledge barriers compound this: limited understanding of PTSD or available services leaves veterans unsure where to start, mistaking symptoms for “normal readjustment.” Comorbid substance use reinforces skepticism, as self-medication seems quicker than uncertain professional paths.
Practical and Access Hurdles
Systemic issues block entry: VA appointment shortages create months-long waits, eroding motivation amid inefficiencies like “red tape” or poor follow-up. Transportation, childcare, work conflicts (30% cite this), or costs deter attendance, especially for rural or senior veterans. Public interaction fears—33-38% report difficulties being out or socializing—make clinic visits daunting.
Demographic variances heighten barriers: Black and non-White veterans face amplified interpersonal challenges; women grapple with school/childcare; older groups worry about time commitments. VHA distrust arises from negative staff experiences or non-therapeutic environments, prompting no-shows.
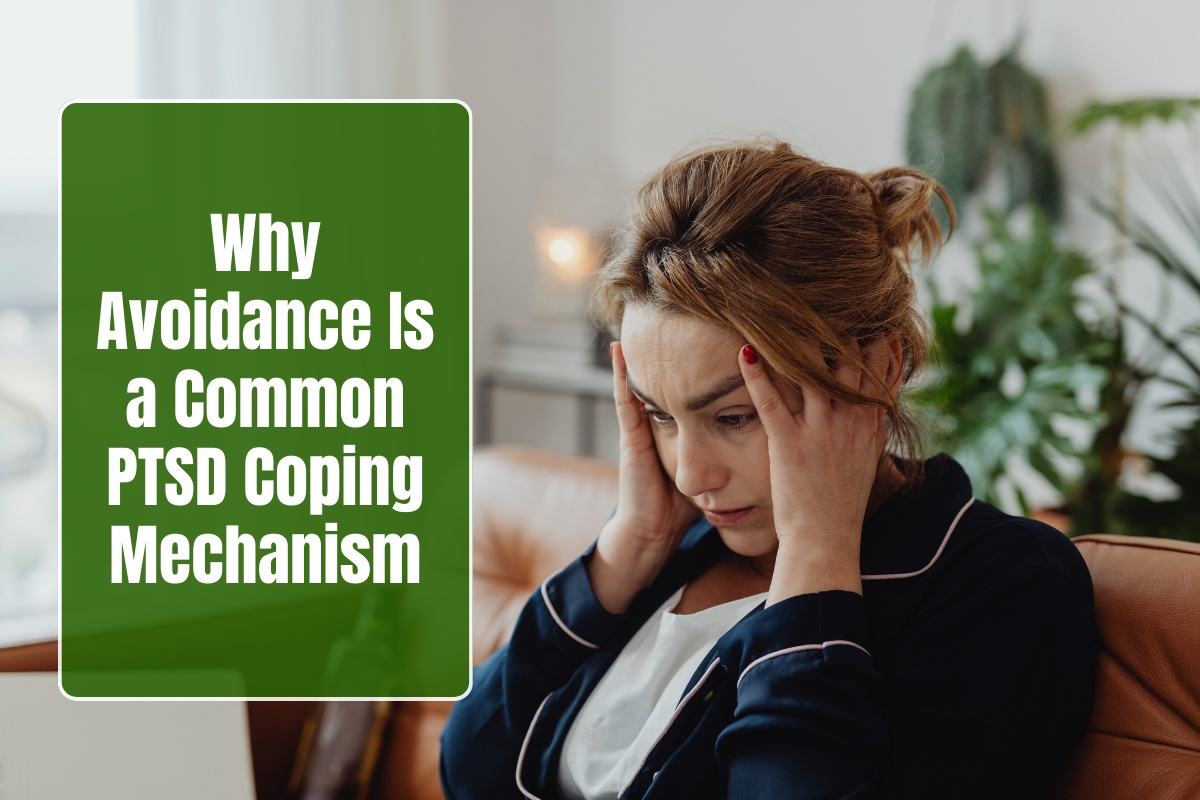
Trauma-Related Avoidance and Emotional Barriers
PTSD symptoms themselves sabotage seeking help: avoidance of trauma memories extends to therapy, where confronting pain feels intolerable. Hypervigilance breeds paranoia about confidentiality, fearing records could harm security clearances or benefits. Pride and values prioritizing stoicism clash with vulnerability required in sessions.
Invalidating homecomings—dismissal as “hero fatigue”—reinforce isolation, while depression saps energy for appointments. Delayed onset masks urgency, with symptoms emerging years later when comorbidities like anxiety solidify avoidance.
Career and Social Repercussions Fears
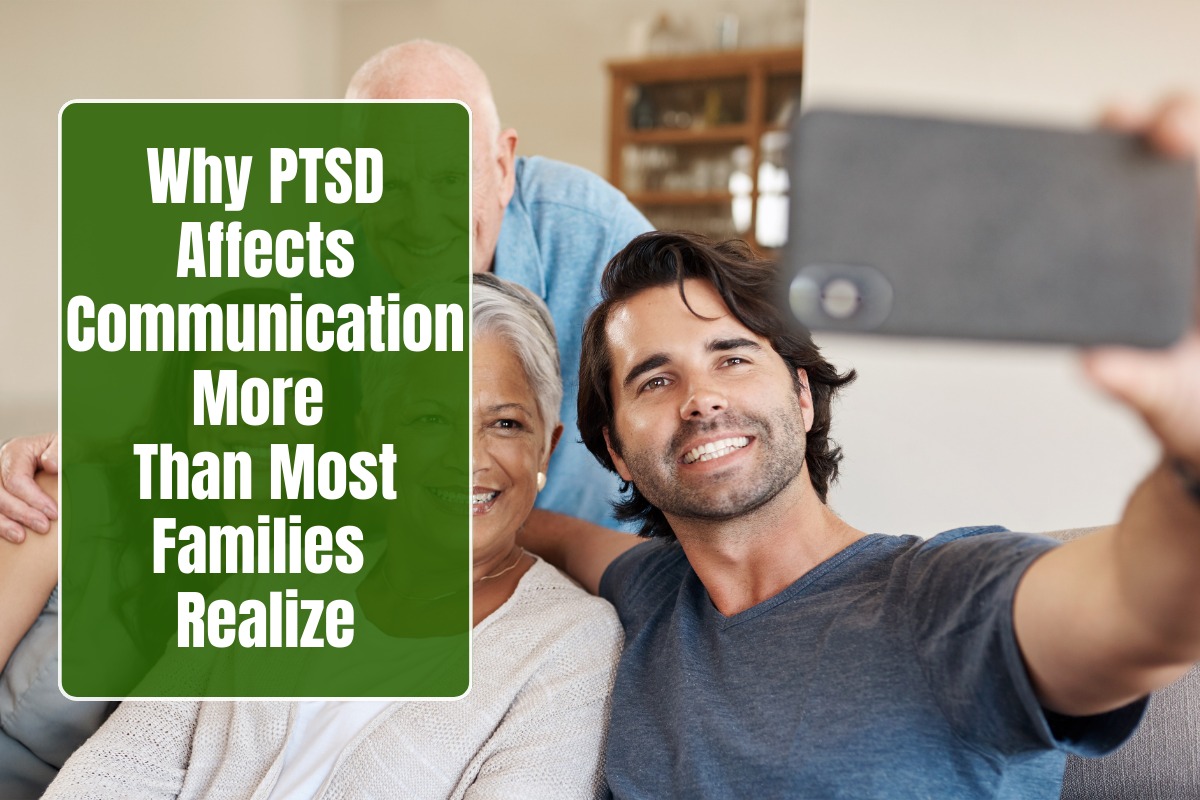
Active and reserve personnel fear repercussions: treatment flags could end careers, limit assignments, or invite profiling. Post-service, stigma lingers via employer bias or benefit concerns, with veterans hiding diagnoses to secure jobs. Family pressures add layers, as partners may unknowingly enable avoidance by managing symptoms at home.
Statistics underscore impact: nearly 40% of suicide veterans lacked diagnoses, partly from untreated PTSD amid barriers; annual costs hit $3 billion for 500,000 cases.
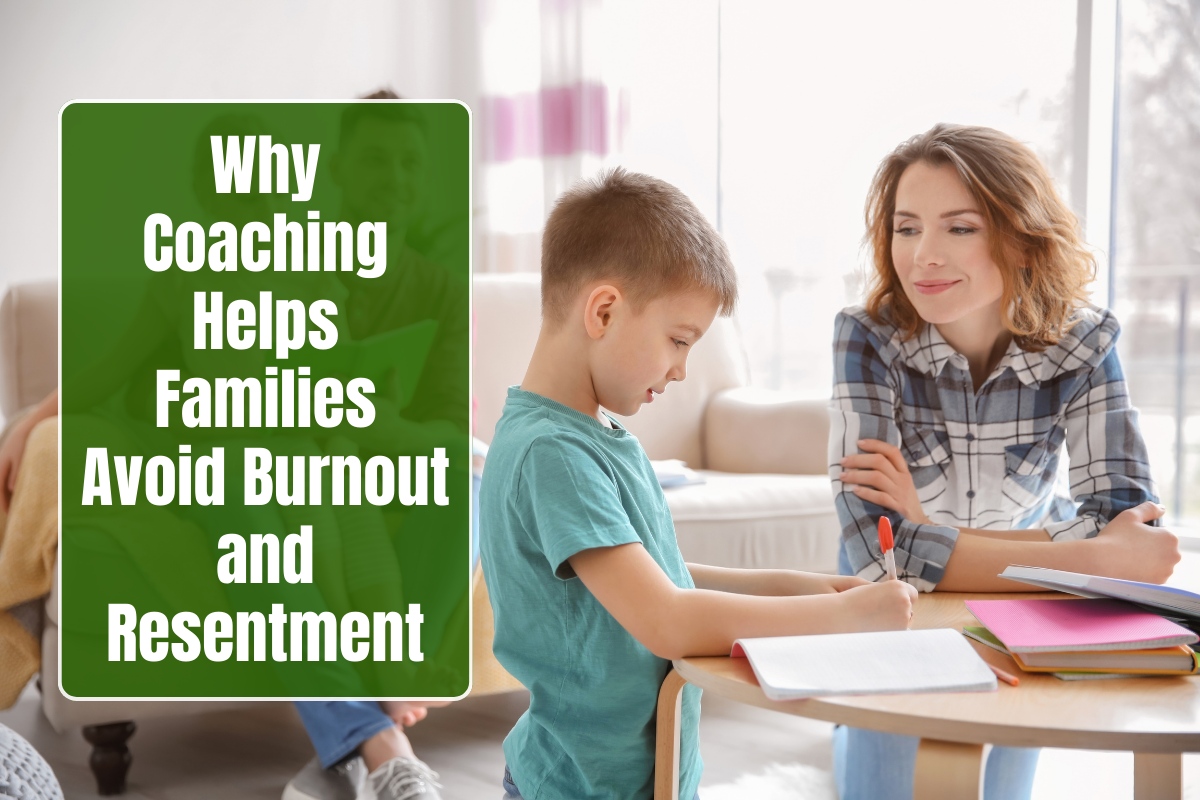
Strategies to Overcome Barriers
Targeted interventions work: peer-led groups normalize help, reducing self-stigma; same-day VA screenings boost follow-through. Telehealth expands access, bypassing travel; education campaigns reframe therapy as mission-focused resilience training. Norms interventions counter perceived stigma by highlighting peers’ positive outcomes. Integrating care with primary services lowers thresholds.
FAQs
Q1: How prevalent is treatment avoidance among veterans with PTSD?
Over 77% report at least one barrier; only 22% face none, with stigma and access topping lists.
Q2: Does military culture uniquely fuel stigma?
Yes, toughness ideals make seeking help seem weak, fearing career harm or peer judgment more than civilians.
Q3: Why distrust VA or therapy effectiveness?
Past delays, inefficiencies, or misinformation lead to beliefs like “it won’t work,” despite evidence-based successes.
Q4: Do PTSD symptoms themselves prevent treatment?
Avoidance of emotions/memories and public fears directly block attendance, creating self-perpetuating cycles.
Q5: How do demographics influence barriers?
Women cite childcare; minorities face interaction issues; seniors worry about time/cost more than youth.
Q6: What reduces these barriers effectively?
Peer support, telehealth, stigma campaigns, and rapid screenings increase utilization by normalizing and easing access.